Products
Customer Reviews
Resources
Support
Chimeric Antigen Receptor (CAR) T cell therapy is a combination of personalized Immunotherapy and gene1. CAR-T cell therapy is a ‘living’ drug established from a patient’s own isolated and engineered T cells. Since the first FDA approval in 2018, CAR-T therapies have achieved 80% in remission rates for hematologic malignancy patients2. As with all adoptive cell therapies, the production of autologous or allogeneic CAR-T therapies is a complicated biomanufacturing process that requires strict adherence to regulatory and QA/QC guidelines. To be ensured the safety, quality, and efficacy of the final product, cell health and viability must be evaluated and monitored throughout the process of development and bioprocessing workflows. Here, we demonstrate how the LUNA-FX7™ may be used to monitor and evaluate cell health at critical stages in the CAR-T process: 1) Collection of the primary source material, 2) Post-Leukapheresis, 3) Isolation / Activation, 4) Expansion, and 5) Production. Curocell Inc., a leading company developing innovative anti-cancer immune therapy in Korea, kindly provided cell count data of two samples randomly selected from each stage of the CAR-T cell production (Figure 1). Cell counts were performed with the LUNA-FX7™ in fluorescent cell counting mode using the nucleic acid stains Acridine Orange and Propidium Iodide (AO/PI, Cat# F23001, Logos Biosystems). In brief, for each count, 2 µl of pre-mixed AO/PI solution was combined with 18 µl of cells, loaded into a 2-, 3-, or 8-channel slide, and counted utilizing the autofocus feature. For the final dosing determinations, the LUNA™ 1-Channel Slides (Cat# L72011) with an analysis volume of 5.1 µl (>10X volume of most automated volumes) were used.
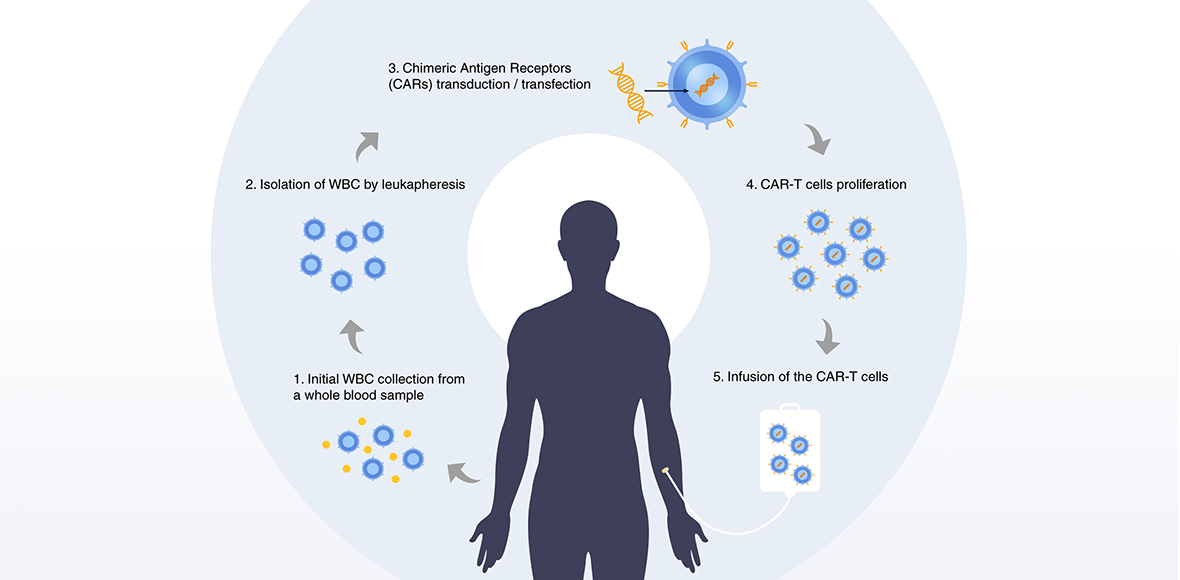
Table 1. Protocol parameter settings for CAR-T cells in Fluorescence Cell Counting mode
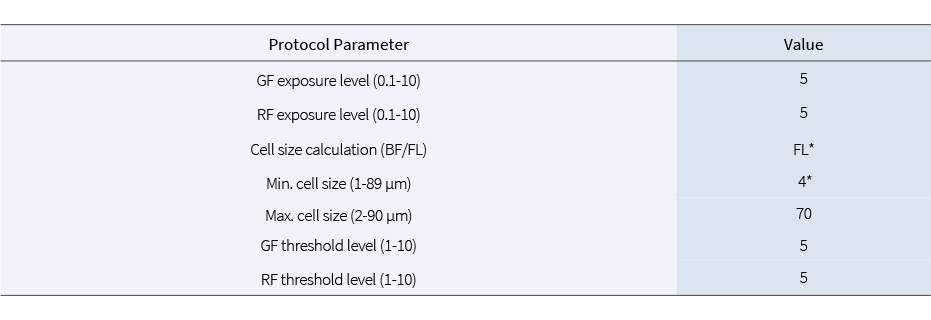
Changed from the DEFAULT values.
Initial WBC concentration and viability from a whole blood sample
After initial blood collection and prior to leukapheresis, cells were diluted 1:100 with 1X PBS for counting in LUNA-FX7™. Despite the fact that white blood cells (WBC) comprise only 2% of a whole blood population, Figure 2 shows how the LUNA-FX7™ can easily differentiate nucleated cells from anucleated cells (i.e. RBC) in a heterogeneous population.
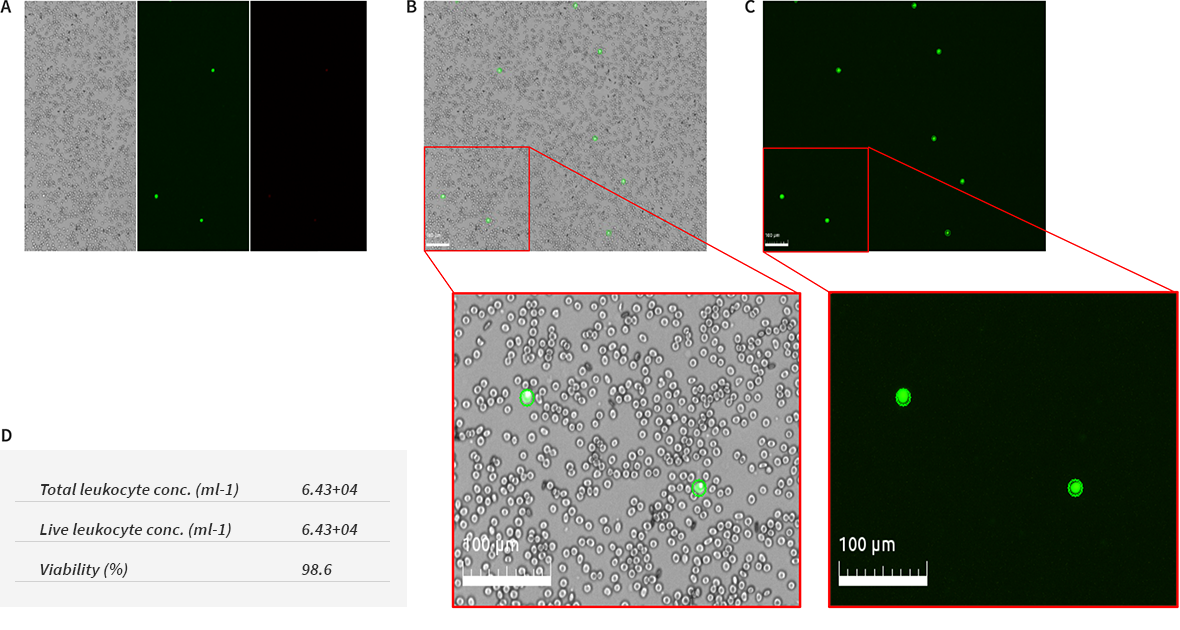
Figure 2. Cell concentration and viability of WBC in whole blood samples. Prior to leukapheresis, a whole blood sample was dilute 1:100 with PBS, stained with AO/PI, and counted. Tiled images of Brightfield (BF), Green channel (GF), and Red channel (RF) (A). Overlay images of tagged (live/dead nucleated cells) images (B, C). Total WBC cell numbers and viability of the 1/100 diluted blood (D). The protocol settings are shown in Table 1.
Leukapheresis is the process of separating WBCs from the whole blood. Figures 3 shows the viability of 2 different samples. RBCs were not seen in either sample, but some cell debris may still be observed. Here again, the LUNA-FX7™ can easily distinguish between cells and cellular or non-cellular debris, minimizing the possibility of counting false positives.
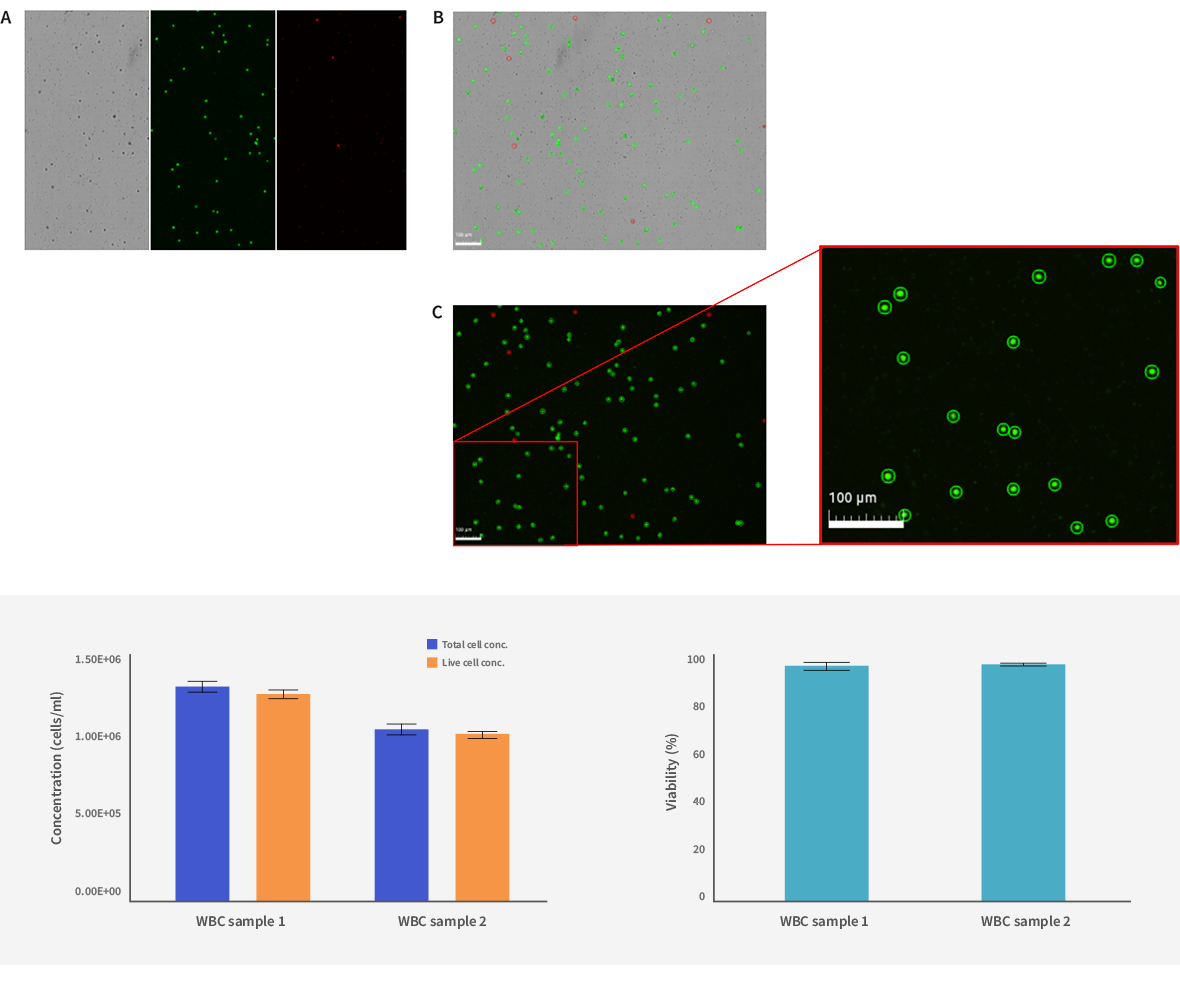
Figure 3. Cell concentration and viability post-leukapheresis. WBC samples counted post-leukapheresis and BF, GF, and RF raw images (A), FL tagged image, and the magnified image (B, C). Two samples were evaluated and the cell concentration and viability were plotted. (D, E). The protocol settings are shown in Table 1.
After leukapheresis, T cells are further isolated and then activated, yielding a homogenous T cell population. At this stage, there is a marked contrast in the quality of samples (Figure 4).
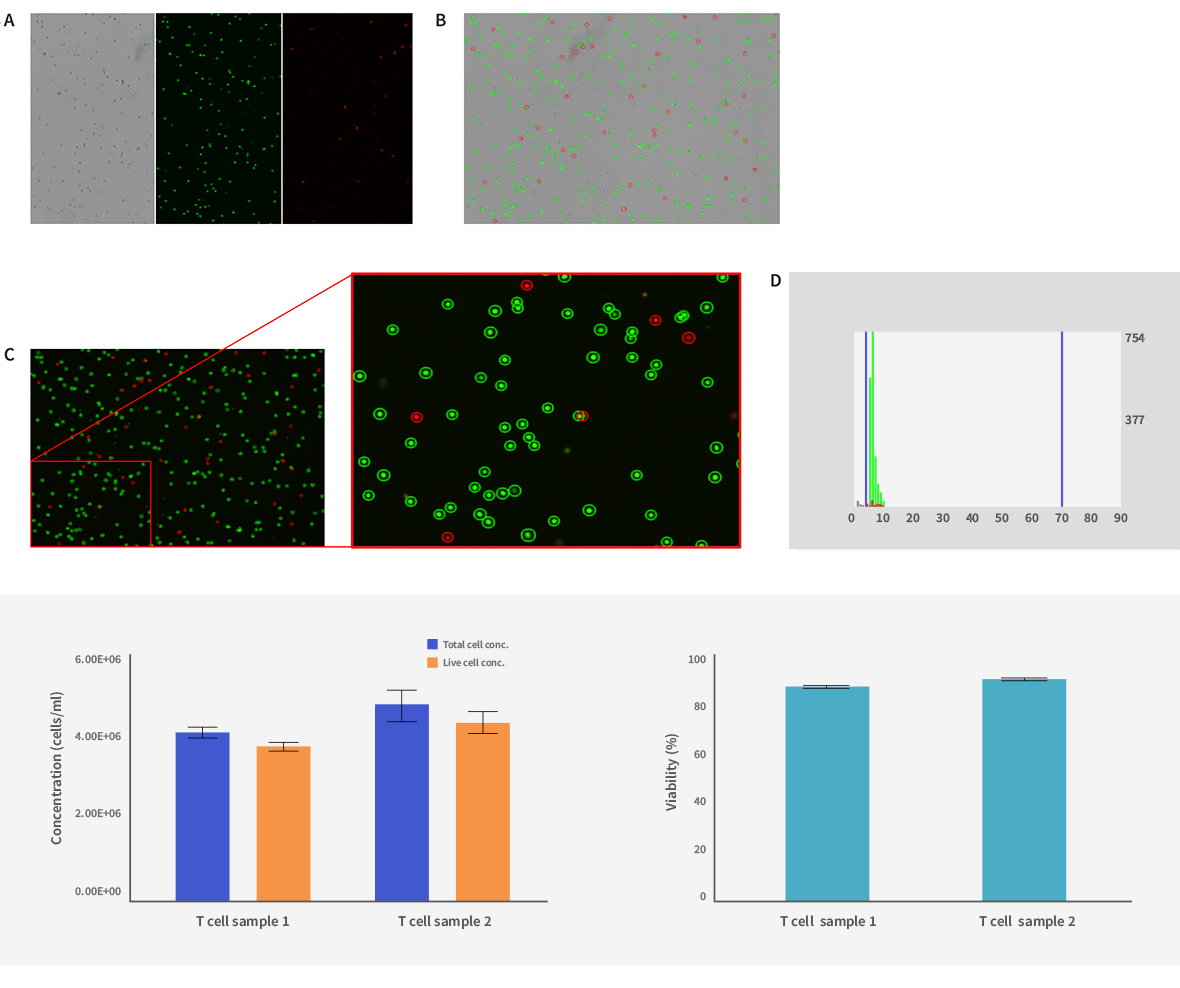
Figure 4. Cell concentration and viability post isolation and activation. T cells were counted post isolation and activation, and BF, GF, and RF raw images (A), and FL tagged image, and enlarged image (B, C). The false-positive debris can be eliminated by a minimum cell size setting (D). Two samples were evaluated and the cell concentration and viability were plotted (E, F). The protocol settings are shown in Table 1.
CARs expressed T cells
The isolated and activated T cells are transduced through retroviruses to produce the chimeric antigen receptors (CARs). After transduction, the newly engineered CAR-T cells are expanded ex vivo. Figure 5 shows cell viability and numbers of expanded CAR-T cells.
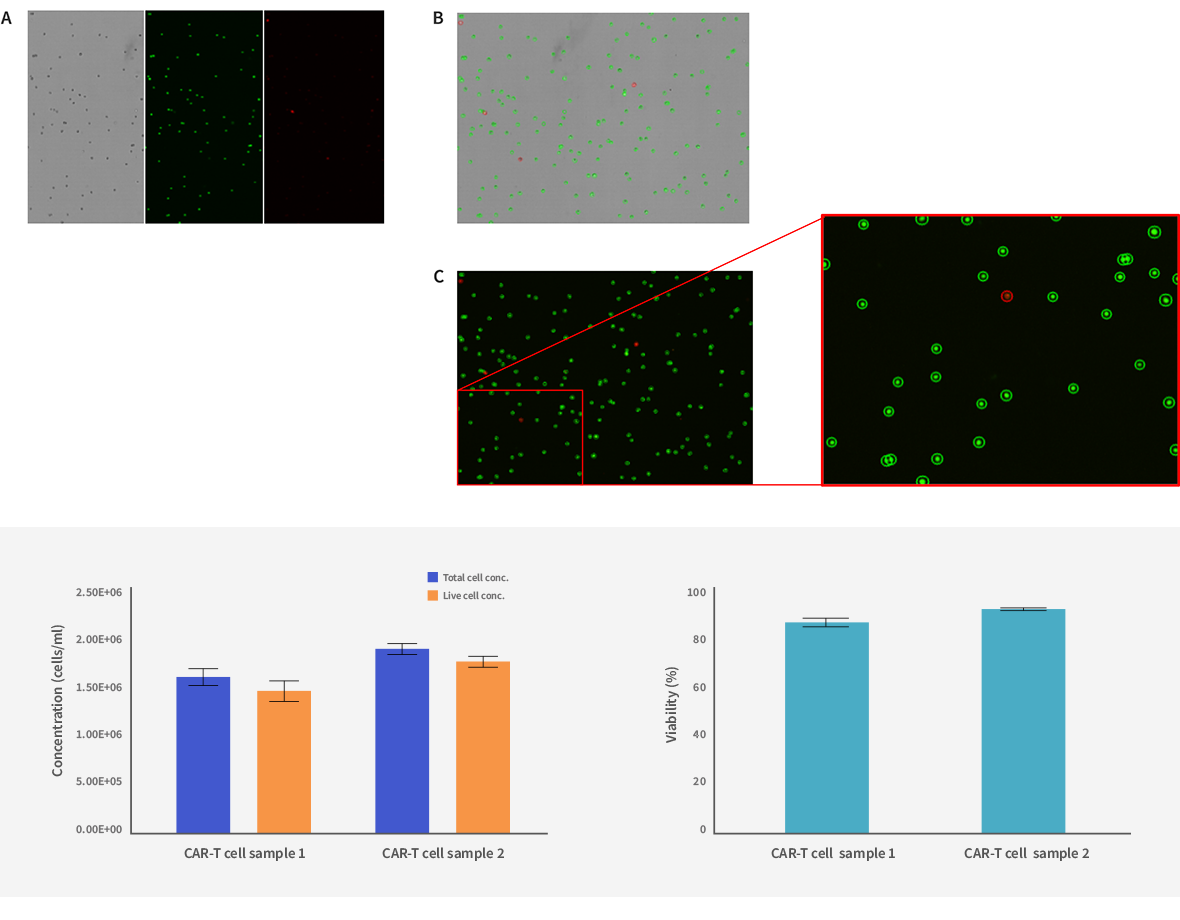
Figure 5. Cell concentration and viability after expansion of CAR-T cells. The raw and tagged images (A, B, C) and the cell concentration and viability (D, E) of CAR-T cell samples. The protocol settings are shown in Table 1.
Expanded CAR-T cells are cryopreserved and evaluated for appropriate dosing. Figure 6 shows the viability and concentration of 2 samples with different cell viability.
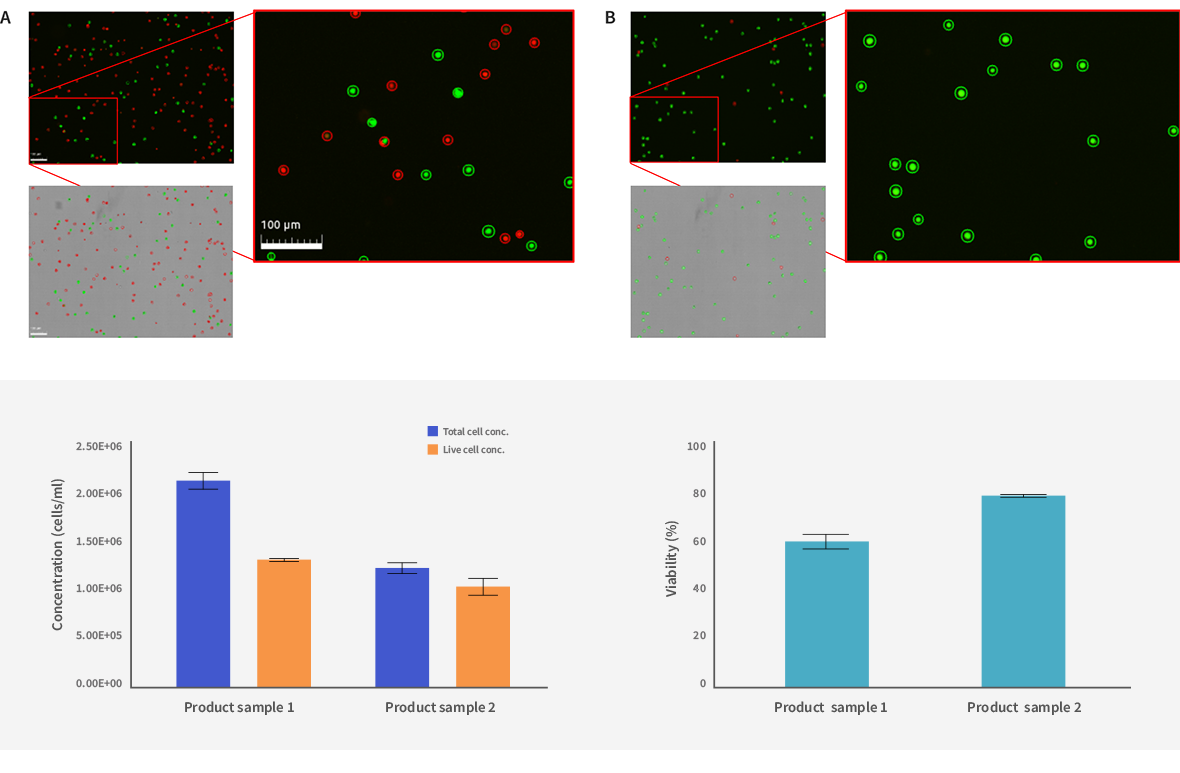
Figure 6. Cell concentration and viability of CAR-T cell final products. Tagged images of the low viability sample (A) and the high viability sample (B) and the corresponding cell concentration and viability (C, D). The protocol settings are shown in Table 1.
From the initial collection of primary source material to final dosing determinations, the LUNA-FX7™ provides the required accuracy and flexibility for monitoring cell health and viability through the entire CAR-T process. Furthermore, in conjunction with pre-set validation slides, internal QC software, and optional 21 CFR Part 11 compliant software ensures that the rigorous QC and regulatory guidelines are met and maintained.
CAR-T Cell Production and Cell Counting with the LUNA-FX7™ This video talks about CAR-T cell therapy and its manufacturing process. At each stage, where cell monitoring is critical, the LUNA-FX7™ Automated Cell Counter is applied, highlighting the advanced functionality and accuracy of the LUNA-FX7™ with CAR-T cell therapy.